



Compact
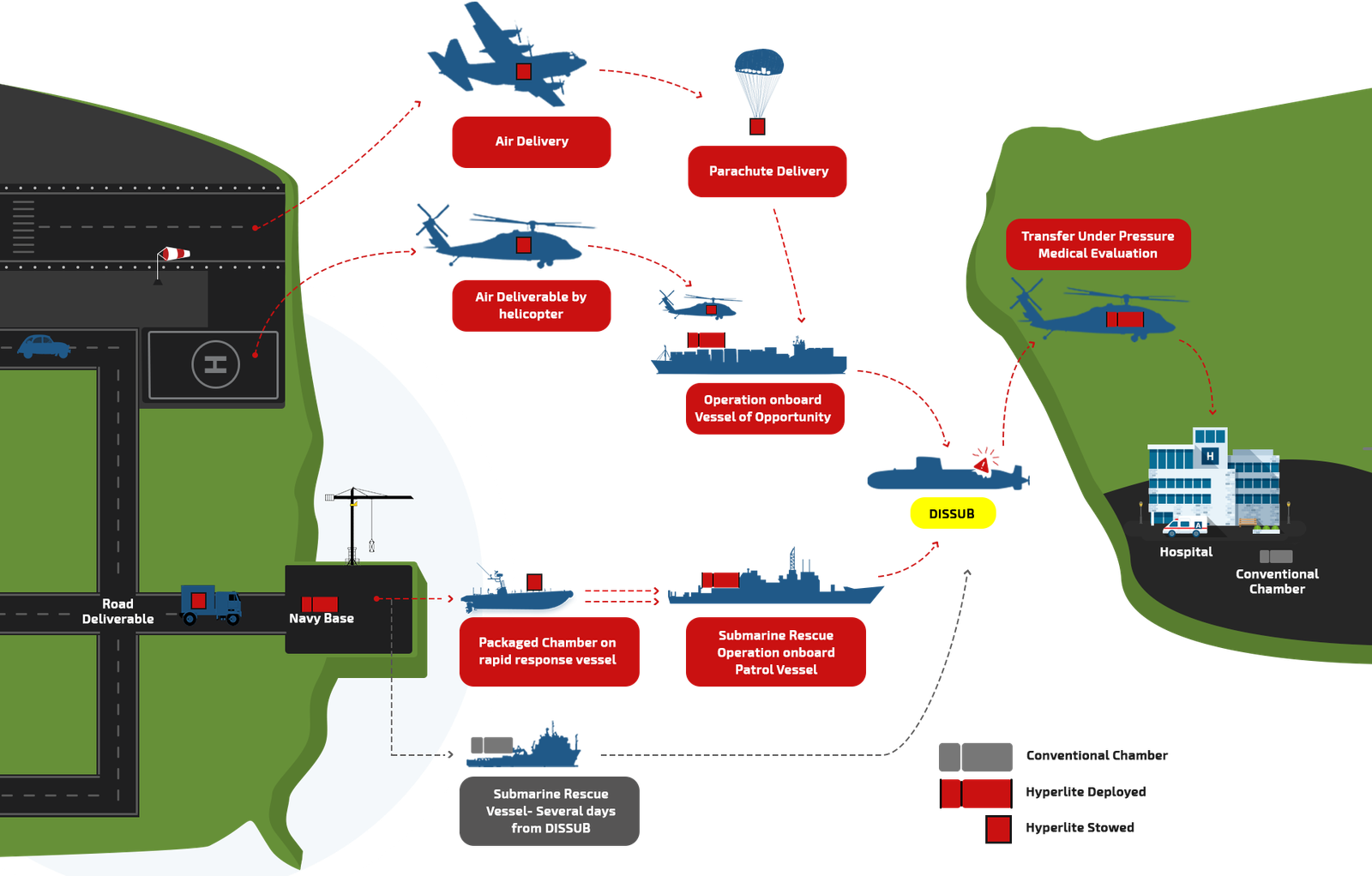
Our compact modular solutions make transportation painless, requiring a small packaged volume, saving valuable space and multiple storage options.
Simple Interface
Our simple control panels and user interfaces are easy to understand and operate.
No Downtime
We offer servicing & maintenance solutions that minimise logistics and keep your system operational 365 days a year.
Portability
Our systems don’t require structural reinforcements or expensive installation on a vessel.




 Occupants: Occupants: |
1 |
 Weight: Weight: |
100kg |
 Max Operating Pressure: Max Operating Pressure: |
2.3 Bar(g) 3.3 ATA |
 Intended Intended Purpose: |
Transfer-Under-Pressure, Emergency Evacuation |


| Occupants: |
2 |
| Weight: |
431kg |
| Max Operating Pressure: |
3 Bar(g) 4 ATA |
| Intended Purpose: |
Full treatment on vessel/site. Designed for use in fixed location. |


| Occupants: |
3-4 |
| Weight: |
>550kg |
| Max Operating Pressure: |
5 Bar(g) 6 ATA |
| Intended Purpose: |
Full Treatment on site. Transportable for Multiple Scenarios |


